Marine animals and plants as omega 3 fatty acids sources


This post is also available in:
This post is also available in:
![]() Español (Spanish)
Español (Spanish) ![]() Deutsch (German)
Deutsch (German) ![]() Ελληνικά (Greek)
Ελληνικά (Greek)
Fats have had a bad reputation because it has been said that excessive consumption of fats leads to higher blood cholesterol and increased risk of heart disease. However, this must be interpreted carefully, as there are different types of fats, which will have different effects on human health. Indeed, the consumption of saturated and trans fats increases the risk of those harmful conditions. But there is another type of fat, unsaturated fats, and within this group, omega-3 fats, which have multiple beneficial attributes, including the opposite effect caused by saturated and trans fats: maintaining good cardiovascular health.
The first indications of the benefits of omega-3 fatty acids were reported in the 1970s in Greenland. The diets of Danish and Greenlandic people living in Greenland were compared. While the Danes had a Western diet, rich in saturated fatty acids from animal sources such as beef and milk, the Greenlanders consumed local marine food, such as seaweed, fatty fish and whale and seal meat, rich in omega-3 fatty acids. The Greenlanders were found to be less likely to suffer from heart disease. This led the scientists to realize that different types of fat have different effects on the body, so the research was directed to investigate these effects further.
What are omega-3 fats?
It is a family of polyunsaturated fats. The main omega-3 fatty acids are:
- Eicosapentaenoic acid (EPA)
- Docosahexaenoic acid (DHA)
- Alpha-linolenic acid (ALA)
How do omega-3 fatty acids work?
The most studied omega-3 fatty acids are EPA and DHA. They come mainly from fish (or marine microalgae) and sometimes are called marine omega-3s. Once ingested, they are rapidly metabolized and have a pronounced anti-inflammatory action by generating anti-inflammatory compounds and blocking the formation of inflammatory compounds. Therefore, EPA and DHA prevent diseases in which inflammation plays a role.
Omega-3 fatty acids and benefits during pregnancy and breastfeeding
EPA and DHA are required for the proper development of the embryo, fetus and baby during their first months, being particularly important for cognitive and vision development, since these fatty acids are in large quantities in brain and photoreceptor cells. It has been reported that the higher the concentration of DHA in the blood of infants, the better their vision and touch-vision coordination, as evidenced by the consumption of DHA by mothers during pregnancy and lactation. Likewise, it was observed that in monkeys that did not receive an adequate supply of omega-3 fatty acids during pregnancy and lactation, the subsequent consumption of EPA and DHA did not improve their vision or their cognitive development. In other words, it is suggested that this benefit of EPA and DHA occurs only when the individual is under development and that, during those stages, deficiency of EPA and DHA deficiency brings irreversible consequences. Therefore, consuming omega-3 fatty acids in pregnant and lactating mothers is highly recommended.
Omega-3 fatty acids for cardiovascular health
Omega-3 fatty acids are crucial for cardiovascular health. Their consumption decreases the total fat content in blood, both in patients with high and normal blood fat content. Likewise, consuming EPA and DHA has an anti-inflammatory effect, key to preventing atherosclerosis, which is the accumulation of plaque inside the arteries. These fatty acids also regulate blood pressure and prevent arrhythmias, which are alterations in the regular heart rhythm. This is explained because EPA and DHA can bind to cardiac cells, thus preventing harmful pro-inflammatory molecules from binding to them.
Omega-3 fatty acids for brain and mental health
The consumption of omega-3 fatty acids is essential for mental health. It has been reported in multiple studies that low levels of DHA in the blood are related to schizophrenia, attention deficit disorder, dyslexia, depression, Alzheimer’s disease and bipolar disorder. This is explained by the fact that the brain is an organ that is composed of large amounts of fat compared to other organs, so the fat that composes it should have healthy and anti-inflammatory effects, like omega-3 fatty acids have.
Other benefits
Other benefits associated with omega-3 fatty acids consumption show that they may reduce arthritis and diabetes. In addition, omega-3 fatty acids can prevent the risk of colon, pancreatic and breast cancer. Lastly, research showed that a higher dietary intake of omega-3’s is associated with a decrease incidence of dry eye disease in women.
Which dietary sources are high in omega-3?
The best dietary sources of EPA and DHA are marine sources, particularly fatty fish such as horse mackerel, sardines, anchovies, tuna and salmon (Figure 1). These fish do not produce EPA and DHA by themselves but obtain it by consuming algae and phytoplankton, the primary sources of EPA and DHA on the planet. Hence, the consumption of algae is also highly recommended.
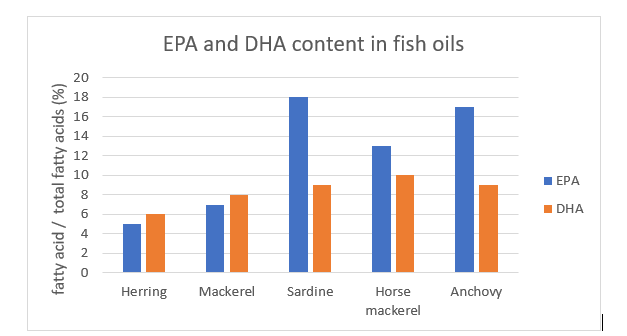
Figure 1. EPA and DHA content in various fish oils (Adapted from Abbas et al., 2009).
Additionally, the amount of total omega 3’s including in some marine sources is presented in Table 1, below:
| Marine source | Omega-3 content (mg/100gr) |
| Mackerel | 4,580 |
| Anchovies | 2,053 |
| Salmon | 2,150 |
| Herring | 2,150 |
| Sardines | 1112 |
| Trout | 1000 |
| Oysters | 391 |
Table 1. Total omega 3 fatty acids content in some marine sources. (Food Data Central, USDA & Harvard)
Which vegetables are high in omega-3?
As for vegetable sources, the best-known omega-3 fatty acid is alpha-linolenic acid (ALA). It is present in significant amounts just in a few vegetable sources: soybean, flaxseed, chia and canola, and in oils derived from them; it is also found in walnuts. Other minor sources are dark leafy greens, kidney beans and edamame. This fatty acid is essential, that is, it needs to be consumed because humans cannot produce it by themselves. ALA is very well absorbed by the body (96% of the consumed ALA is absorbed), where it will have multiple destinations: to be part of the adipose tissue, to provide energy, to be transformed into the beneficial omega 9 fatty acids, and the most important: to be transformed into the widely studied and previously detailed EPA and DHA.
Omega-3’s and its (undesired) interaction with omega-6’s
However, the transformation of ALA to EPA and DHA is affected by the consumption of omega-6 fatty acids, such as linoleic acid. For humans, only two fatty acids are essential: ALA and linoleic acid. Linoleic acid also has important functions in the body, but when consumed in large amounts it produces pro-inflammatory metabolites that in the long term will cause cardiovascular disease, osteoporosis and certain types of cancer. In most plant sources, linoleic acid far outweighs ALA (Table 2), so in modern Western diets the ratio of omega-6/omega-3 fatty acid intake is grossly imbalanced in favor of omega-6, which may explain the origin of many conditions and diseases. Also, when linoleic acid is consumed, it will require the same enzymes that ALA requires for its metabolism, so there will be competition between linoleic acid and ALA for these enzymes. Thus, with a much higher intake of linoleic acid, the metabolism will be in favor of the latter, generating harmful pro-inflammatory metabolites and not producing healthy EPA and DHA. Therefore, it is recommended to increase the consumption of seafood, rich in EPA and DHA, and to decrease the excessive consumption of omega-6 fatty acids, which are also important, but whose unbalanced consumption is the cause of several health problems.
| Oil / fatty acid | Linolenic (omega 6) (%) | α-linolenic (omega 3) (%) |
| Olive | 7 | 1 |
| Maize | 52 | 1 |
| Soybean | 53 | 8 |
| Sunflower seed | 60 | 0 |
| Cottonseed | 56 | 0 |
| Wheat germ | 60 | 5 |
| Canola | 14 | 10 |
| Palm | 12 | 0 |
| Sesame | 46 | 0 |
Table 2. Comparison of linoleic acid (omega 6) and α-linolenic acid (omega 3) content in various vegetable oils, expressed as % of fatty acid with respect to total fatty acids. (Yildiz et al., 2010).
It could be recommended to consume more ALA, in addition to EPA and DHA. However, this solution is partial, since the conversion of ALA to EPA and DHA is very poor: of the total ALA consumed, just 5% is converted to EPA and less than 1% is converted to DHA. Therefore, the best solution is not to consume foods rich in ALA, i.e. not to consume the precursor of EPA and DHA, but to consume foods rich in EPA and DHA directly. So, let’s increase the consumption of fish and algae in our diet!
What is the recommended daily dose?
The American Heart Association suggests eating fish, or other seafood (170-230gr) at least twice a week as part of a healthy diet (for people with no coronary disease). This provides an average consumption of EPA and DHA of 250mg per day. Other institutes and health professionals recommend taking 250-1000 mg per day.
The Global Organization for EPA and DHA Omega-3s reported that the recommended intakes of EPA and DHA differ among the countries. For example, the daily intake recommendation in Russia is 1300mg, and in France and Norway is 450mg. In most European countries, the recommendation intake is 250mg. In other countries, such as New Zealand and Australia is even lower, at 160mg.
For people following a plant-based diet, the adequate intake is 1,600mg for males and 1,1100mg for females, according to the National Institute of Health (USA).
References:
- Abbas, K.; Mohamed, A.; Jamilah, B. (2009). Fatty acids in fish and beef and their nutritional values: a review. Journal of Food, Agriculture and Environment, 7 (3), 37-42.
- C. Burdge (2006). Metabolism of α-linolenic acid in humans. Prostaglandins, Leukotrienes and Essential Fatty Acids, 75(3), 0–168. doi:10.1016/j.plefa.2006.05.013
- Harris, Kristina A. B.A.; Hill, Alison M. Ph.D.; Kris-Etherton, Penny M. Ph.D., R.D. (2010). Health benefits of marine-derived omega 3 fatty acids. ACSM’s Health & Fitness Journal 14(2):p 22-28. DOI: 10.1249/FIT.0b013e3181cff40fSujatha Rajaram. (2014). Health benefits of plant-derived α-linolenic acid, The American Journal of Clinical Nutrition, Volume 100, Issue suppl_1, Pages 443S–448S, https://doi.org/10.3945/ajcn.113.071514
- Natalie D. Riediger; Rgia A. Othman; Miyoung Suh; Mohammed H. Moghadasian (2009). A Systemic Review of the Roles of n-3 Fatty Acids in Health and Disease. Journal of the American Dietetic Association, 109(4), 668–679. doi:10.1016/j.jada.2008.12.022
- Aliza H Stark, Michael A Crawford, Ram Reifen. (2008). Update on alpha-linolenic acid, Nutrition Reviews, Volume 66, Issue 6, 1, Pages 326–332, https://doi.org/10.1111/j.1753-4887.2008.00040.x
- Valenzuela, R.; Tapia, G.; González, M.; Valenzuela, A. (2011). Ácidos grasos omega-3 (EPA y DHA) y su aplicación en diversas situaciones clínicas. Revista Chilena de Nutrición, 38 (3), 356-367.
- Yildiz, F. (2010). Advances in food biochemistry. First edition. CRC Press, Taylor and Francis Group. Boca Raton, Florida, The United States of America.